

Abstract
BACKGROUND:
Systemic immunosuppression (SIS) is the standard treatment for significant acute and chronic graft versus host disease (GVHD) after allogeneic hematopoietic cell transplantation (HCT). Previous studies have shown that 30-70% of patients require immunosuppressive treatment for GVHD for more than 2 years. Prolonged SIS increases the risk of infections, recurrence of malignancy and multi-organ complications including endocrine dysfunction, hypertension, myopathy and ocular complications. This study aimed to evaluate the predictive factors associated with increased likelihood of SIS discontinuation from 3 different time points: from the day of transplant in all patients, from the day of treatment of acute GVHD (aGVHD) and from the day of treatment of chronic GVHD (cGVHD).
METHODS:
A retrospective review was conducted in 674 consecutive patients who underwent allogeneic HCT at Princess Margaret Cancer Centre from 2004 to 2013. Analyses were done using cumulative incidence method considering competing risks for SIS discontinuation. The incidence of SIS discontinuation was calculated from 3 time points: from the day of transplant in all patients, from the day of treatment of aGVHD and from the day of treatment of cGVHD. Univariate and multivariate analyses were conducted to identify the predictive factors for SIS discontinuation and hazard ratio (HR) with 95% confidence interval (CI) was calculated using Fine-Gray model.
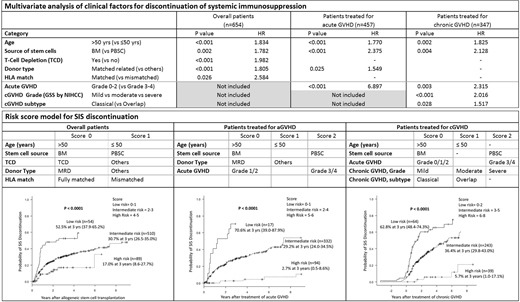
Risk score models were generated based on the results from the multivariate analysis with respect to the 3 time points. Each predictive factor was weighted according to the HR. Risk score models are presented in the Table below: for each risk score model, the patients were divided into 3 risk groups based on the scores. The cumulative incidence of SIS discontinuation was compared according to the risk group for each risk score model as shown in the Figure below.
RESULTS:
With a median follow-up duration of 3.5 years, the probability of SIS cessation at 3 years was 30.7% (27.0-34.5%) in all patients (n=674), 25.4% (21.2-29.8%) in patients treated for aGVHD (n=457) and 34.6% (29.1-40.3%) in patients treated for cGVHD (n=347).
Multivariate analysis confirmed the following predictive factors associated with increased likelihood of SIS discontinuation. In all patients (n=654): age >50 years (vs ≤ 50 yrs; p<0.001, HR 1.83), bone marrow (BM) as a source of stem cells (vs peripheral blood [PBSC]; p=0.002, HR 1.78), T-cell depletion (vs no T-cell depletion; p<0.001, HR 1.98), matched related donor (vs others; p<0.001, HR 1.81) and HLA match (vs partially mismatched HLA; p=0.026, HR 2.58). In patients treated for aGVHD (n=457): age>50 (vs ≤ 50 yrs; p<0.001, HR 1.77), BM (vs PBSC; p<0.001, HR 2.38), matched related donor (vs others; p=0.025, HR 1.55) and aGVHD grade 0-2 (vs grade 3/4 aGVHD; p<0.001, HR 1.77). In patients treated for cGVHD (n=347): age >50 (vs ≤ 50 yrs; p=0.002, HR 1.83), BM (vs PBSC; p=0.004, HR 2.13), Grade 0-2 aGVHD (vs grade 3/4 aGVHD; p=0.003, HR 2.32), cGVHD grade (mild vs moderate vs severe; p<0.001, HR 2.02) and classical subtype (vs overlap syndrome; p=0.028, HR 1.52).
The risk score model stratified the patients into low, intermediate and high risk groups: for all patients, SIS discontinuation at 3 years was 52.5% (37.9-65.2%), 30.7% (26.5-35.0%) and 17% (8.6-27.7%) respectively (p<0.0001); in patients treated for aGVHD, SIS discontinuation at 3 years was 70.6% (39.0-87.9%), 29.2% (24.0-34.5%) and 2.7% (0.5-8.6%) respectively (p<0.001); in patients treated for cGVHD, SIS discontinuation at 3 years was 62.8% (48.4-74.3%), 36.4% (29.8-43.0%) and 5.7% (1.0-17.1%) respectively (p<0.001).
CONCLUSIONS:
Older age, bone marrow as a source of stem cells, T-cell depletion, matched related donor and a full matched donor increase the likelihood of discontinuation of SIS after allogeneic HCT. In addition, the severity of aGVHD and cGVHD significantly affects the chance of SIS discontinuation. The proposed risk score stratifies patients into well-defined groups according to the chance of SIS discontinuation. Further studies in a larger number of patients are strongly recommended to validate this finding. Prospective validation is also warranted to confirm the utility of the risk score as a clinical tool for estimation of likelihood of SIS discontinuation in patients after allogeneic HCT.
Lipton:Pfizer: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal